
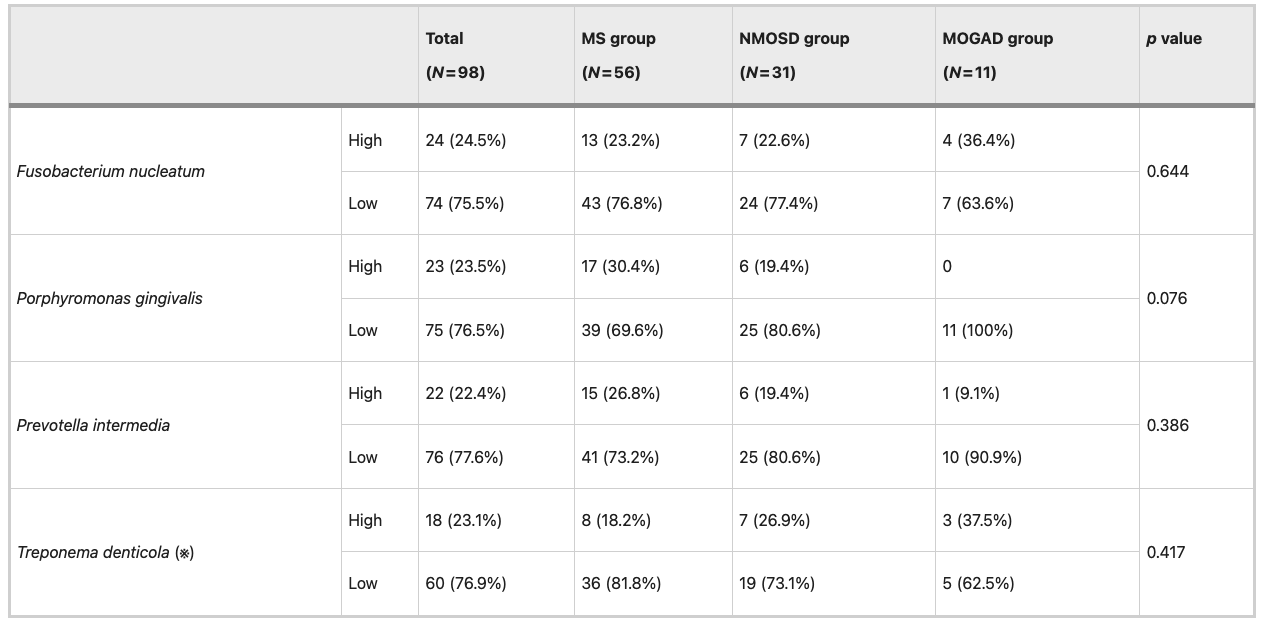
New research links oral bacteria to disability severity in MS, pointing to a possible “oral–brain axis” (Table 1).
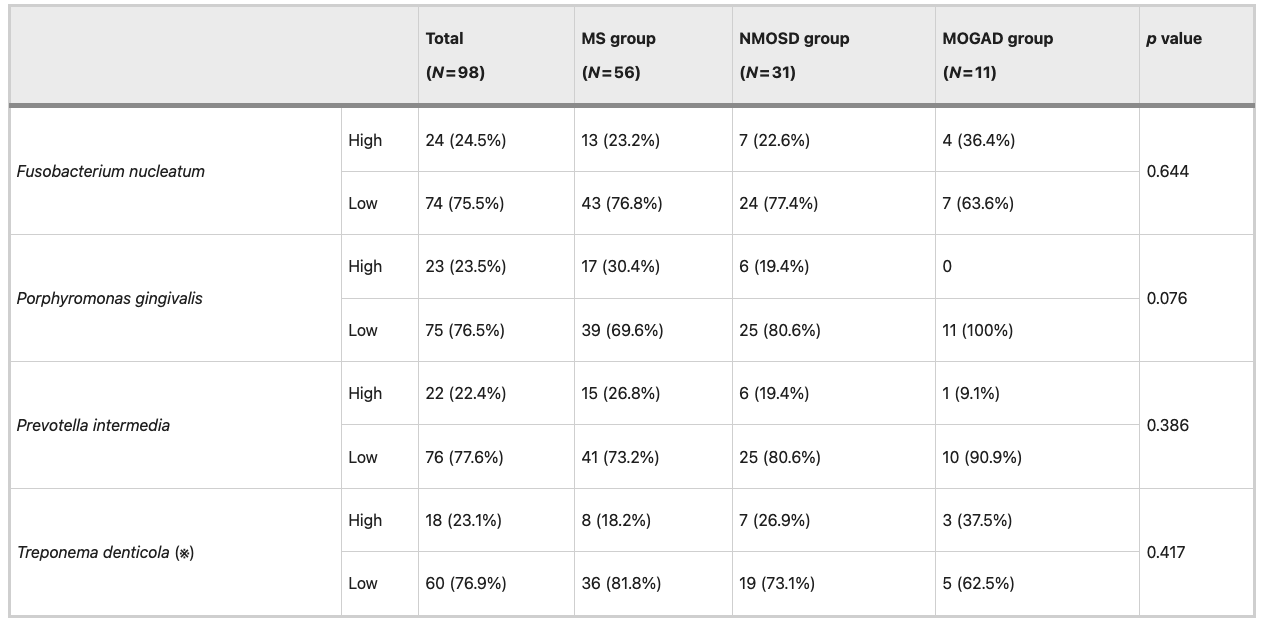
Table 1: Proportion of patients with high and low relative abundances of periodontal pathogens stratified by central inflammatory demyelinating disease. MS, multiple sclerosis; NMOSD, neuromyelitis optica spectrum disorder; MOGAD, myelin oligodendrocyte glycoprotein antibody-associated disease. High and low abundances were defined using the third quartile (Q3) cutoff for the ΔΔCt-calculated relative abundance. High = top 25%, low = below Q3. (※) For Treponema denticola, the total number of evaluated patients was lower than the total number of patients in each disease group because several samples did not yield valid Ct values by qPCR and were thus considered nondetectable. As a result, the total number of patients evaluated for this pathogen was 78 (MS patients 44; NMOSD patients 26; MOGAD patients 8).
- Multiple sclerosis (MS)
- Neuromyelitis optica spectrum disorder (NMOSD)
- Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD)
- MS patients with high levels of Fusobacterium nucleatum were far more likely to have EDSS ≥ 4, indicating moderate to severe disability
- After adjusting for age, disease duration, relapse history, and MS subtype, these patients had ~10-fold higher odds of severe disability
- Nearly 62% of MS patients with high F. nucleatum levels had moderate-to-severe disability, compared with ~19% of those with lower levels
- Could improved oral hygiene or periodontal treatment slow disability progression?
- Might oral bacteria serve as biomarkers for disease severity or progression risk?